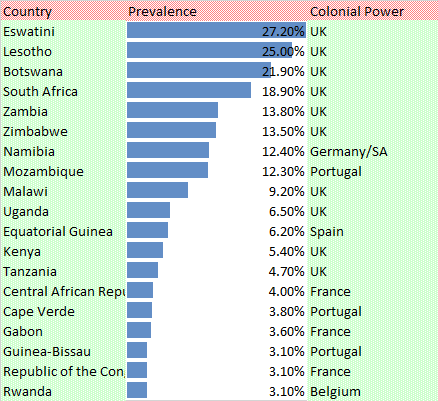
In other words, what is so different about sexual behaviour in Morocco, where HIV prevalence is less than 0.1%, and that in Eswatini (Swaziland), where it is 27.2%, 272 times higher?
As an example at the subnational level, what is so different about sexual behaviour in the Kenyan county of Wajir, where prevalence is less than 0.1% and the county of Siaya, where prevalence is 21.0%, over 200 times higher?
Petabytes of data have been collected about sexual behaviour all over the world. Everywhere, some people have a lot of sex, some people have little or none and the rest are somewhere in between. But few useful correlations between heterosexual behaviour and HIV transmission have been found, at national or sub-national levels.
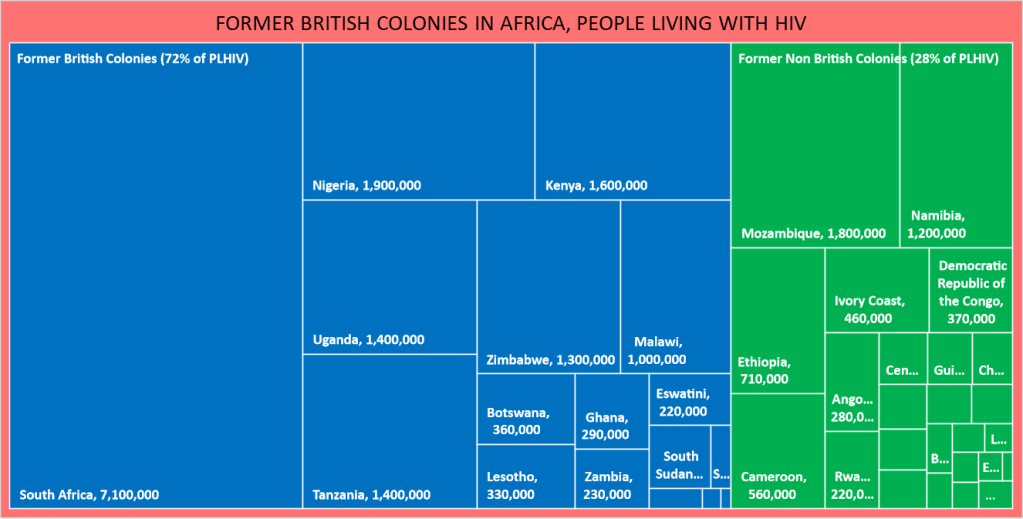
At the national level, the majority of the highest prevalence countries, and the countries with the largest number of people living with HIV are former British colonies. Prevalence ranges from 0.1% (Egypt) to 27.2% (Eswatini), with a median of 6.5% (Uganda).
Data Source: UNAIDS
In contrast, the range in former non-British colonies is 0.1% (Algeria and Tunisia) to 12.4% (Namibia). The median is about 1.5%. A third of these countries have prevalence figures of 1% or below. Less than one third of people living with HIV live in former non-British colonies.
Data Source: UNAIDS
The copious quantities of sexual behavior data referred to above confirm that the British did not introduce a liberal or enlightened attitude towards sex, nor did they promulgate forms of ‘risky’ sexual behaviour not found in French or Belgian colonies. So there must be something unrelated to sex involved, right?
Although modes of HIV transmission have been identified, it seems likely that the contribution of non-sexual transmission via unsafe healthcare and other skin-piercing processes in sub-Saharan African countries has been seriously underestimated by UNAIDS and the other recipients of massive HIV funding.
Currently, people in sub-Saharan Africa receive incessant warnings about sexual risks, with non-sexual risks through unsafe healthcare and other skin-piercing processes dismissed as minor. And although risks of bloodborne infection, especially in healthcare facilities, were identified and addressed in wealthier countries from the 1980s, there have been many outbreaks in poorer countries later shown to be a result of unsafe healthcare.
There are examples of bloodborne HIV outbreaks that have been investigated and confirmed to have been a result of unsafe healthcare. One in Ratodero, Pakistan, is currently being investigated. There was a recent one in Roka Commune in Cambodia that was also investigated. Outbreaks in Romania, China and other countries received international press attention.
However, no bloodborne outbreaks in sub-Saharan Africa have been investigated. Instances that should have been seen as possible bloodborne outbreaks have been ignored. But lurking in the history of healthcare development and practices in Africa, both pre- and post-independence, may be a clue as to why HIV should be so prevalent in former British colonies.


Pingback: Hyperendemic HIV: a WASP factor? | Bloodborne HIV: Don't Get Stuck!