More than two thirds (69%) of PLHA globally live in countries that were either colonized by the British or were heavily influenced by them. India, Brazil, United States, Bahamas, Indonesia and Thailand are the only non-African countries that appear in the top 20, with India and United States being former British colonies.
Similarly, 11 of the top 20 countries for
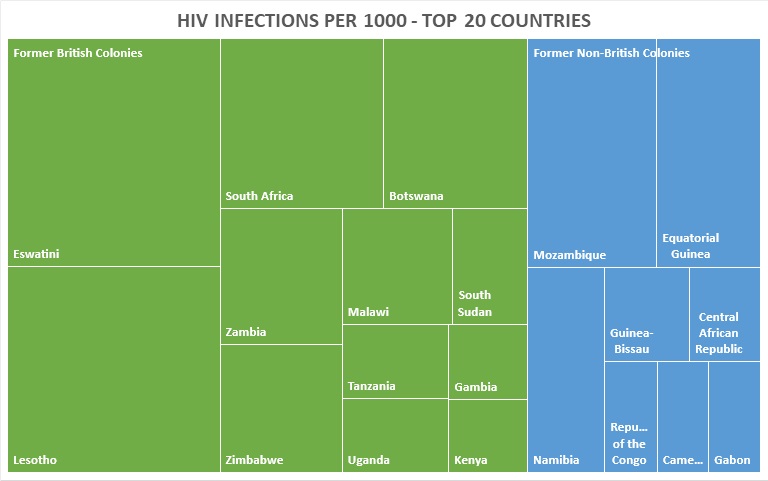
HIV prevalence are former British colonies; the number goes up to 12 if you
include Namibia, whose history, politics, administration, infrastructure, etc,
have arguably been more shaped by British than by German or South African
influences.
Several figures that were not used in the previous post have now been tabulated. Almost two thirds (65%) of annual new HIV infections occur in countries with these overlapping histories. Out of the top 20 countries for new HIV infections per 1000 uninfected people, 12 of them fall into this category.
Although I have not prepared the figures for morbidity by religion, the figures presented show that many of the countries with a predominantly non-Catholic Christian population are also most affected by HIV. In contrast, many of the countries with a predominantly Catholic population (for example, former French, Belgian and Spanish colonies) are less affected by HIV.
Mozambique, alone, stands out as the only one in the top 10 countries by prevalence which was not colonized or strongly influenced by British colonialism. Catholicism is also the biggest religion there, at nearly 30% of the population.
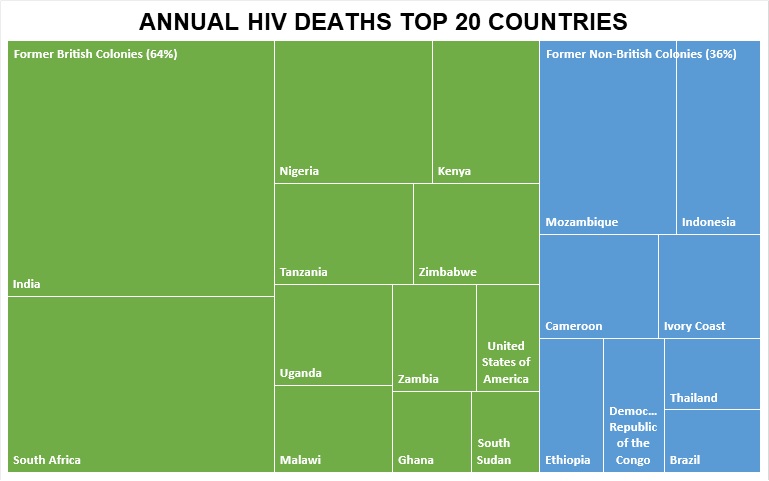
Another figure not included in the previous blog on this subject is for HIV deaths. Just under two thirds of annual deaths (64%) are accounted for by countries previously colonized or heavily influenced by the British.
The table below summarizes the above
findings. The top 20 countries account for 81% of new HIV infections, globally,
and also 81% of PLHA globally.
The thrust of this site is that HIV
epidemics, especially in some sub-Saharan Africa countries, are likely to be
driven more by unsafe healthcare and other bloodborne modes of transmission,
and less by the ‘unsafe’ sexual behaviour that big HIV institutions would have
us believe.
The above data makes no attempt to suggest that there is such thing as ‘WASP-influenced’ sexual behaviour; the received view that 80-90% of HIV transmission is a result of sexual behaviour, but only in the most affected countries, is not founded on evidence.
But the data may show that there is something about certain healthcare infrastructures and/or healthcare administrative structures that explains why the bulk of HIV morbidity and mortality, globally, occurs in countries formerly colonized by the British, or heavily influenced by the British.
The aim of HIV research and analysis should
be to prevent further transmission of the virus, not to point the finger at who
or what is driving epidemics. But as long as UNAIDS and other HIV focused
institutions choose to blame the victims and point the finger at their ‘unsafe’
sexual behaviour, BloodborneHIV.com will continue to search for patterns that
emerge from those same institutions’ data.