It’s refreshing to experience a work of drama that describes a HIV outbreak which occurs in a healthcare setting, without a hint of the prurience that is so common in most accounts of the subjects of HIV and Aids. The play closes tomorrow in the Hampstead Theatre in London (review).
The King of Hell’s Palace tells the story of Dr Shuping Wang, who risked her life, and the safety of her family and friends, to raise awareness of exceptionally high rates of HIV transmission in Henan Province, China, in the 1990s. These were evidently a result of unsafe practices in plasma donation programs, which were a source of income for hundreds of thousands of people in the province.
Estimates of how many people were infected with HIV and hepatitis C through these programs vary, from 10s of thousands to hundreds of thousands, and it’s impossible to say how many were infected. It’s also likely that many of those infected by the plasma programs went on to infect others, directly and indirectly.
Dr Shuping Wang succeeded in closing down
the plasma donation programs. Safety procedures were put in place before they
were allowed to restart. An awful lot of damage was done, and those who were
benefiting most from the programs were reluctant to see their source of income
threatened. But the efforts of one person undoubtedly saved hundreds of
thousands of people, perhaps millions.
Most people who watch movies will have seen
movies that have been made about HIV and Aids. But the bulk of them are about
HIV transmission among men who have sex with men. Some bring in injected drug
use, and some include transmission among heterosexuals, especially where sex
workers are involved.
However, most HIV positive people in the
world are not sex workers, they are not men who have sex with men, they don’t
inject drugs and most of them are certainly not white people from wealthy
countries.
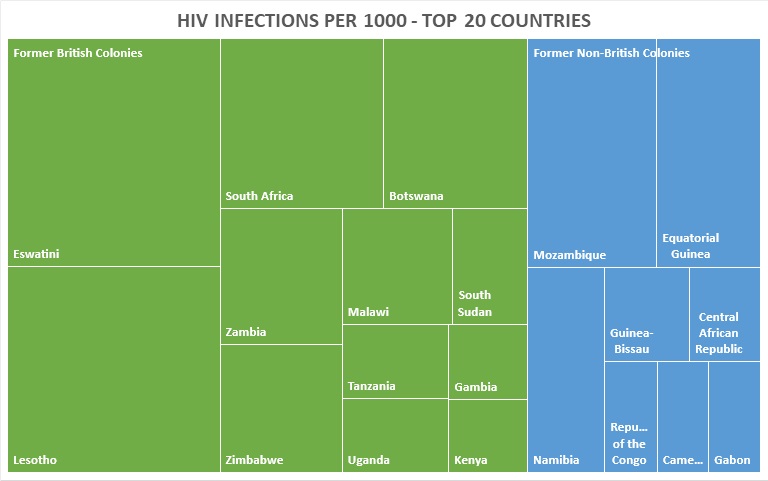
The majority of HIV positive people live in
certain parts of certain sub-Saharan African countries. In other words, they
are not distributed evenly among populations, as you might expect of a virus that
is, according to the HIV industry, almost always transmitted via ‘unsafe’ sex.
Most people in all countries in the world, African countries included (surveys of sexual and other behaviors), do not engage in the very high levels of ‘unsafe’ sex that would be required to account for massive outbreaks that are found in countries such as South Africa, Botswana, Eswatini (Swaziland) and Lesotho.
Some people in all countries in the world do engage in high levels of ‘unsafe’ sex, but most do not. In fact, even among sex workers in wealthier countries, HIV prevalence is low unless they also have other risks, such as injecting drugs.
What you do find in African countries is
unsafe healthcare, badly trained healthcare professionals, quacks and low
skilled practitioners who pass themselves off as doctors, nurses and midwives,
dispensaries that will give you anything if they can make money out of it,
including injections of things you don’t need, and that may do more harm than
good.
And yet there has never been a single investigation in sub-Saharan Africa of the kind that closed down the unsafe plasma programs in China in the 90s. There were investigations in Pakistan (still going on), Cambodia, Libya, Russia, Tajikistan and a number of other countries (list of countries which have and have not responded to outbreaks).
The Chinese administration officials in 1990s Henan Province are depicted as greedy, and as being unwilling to risk losing their job and reputation, even though they knew that Dr Suping Wang was right; they were infecting countless people with deadly pathogens just so they could cash in on the demand for plasma.
Similarly, there are officials in UNAIDS
and other UN offices, such as the WHO, officials in the CDC, various country
administrations in high HIV prevalence countries, academics all over the world
and even journalists who see themselves as having a role in highlighting
serious injustices; why are they not calling for investigations into outbreaks
that affect more than half of young women in some towns in South Africa,
Western Kenya, parts of Tanzania, Mozambique and Malawi?
There have been protests and movements
demanding rights for men who have sex with men, transsexuals, and others in
wealthy countries, where the majority of HIV positive people fall into those
groups.
But where the majority of HIV positive
people are black, and they are neither men who have sex with men nor injecting
drug users (HIV positive females outnumber HIV positive males in high
prevalence countries), there are no protests.
About 70% of HIV positive people live in
sub-Saharan Africa and over 70% of HIV positive people in the region live in certain
towns and cities in just a handful of countries: that’s where the
investigations need to be carried out. Surely, no one’s interest is served by
continuing to insist that HIV prevalence is high in a few places just because
of ‘African’ sexual behaviour?