According to Avert.com “more than $400 million [of donor funding] was committed to HIV and AIDS in 2007/2008“. However, less than a quarter of that funding, probably around 20%, was spent on ‘prevention’, with the usual assumption that almost all HIV is transmitted through heterosexual behavior. Around 60% is estimated to have been spent on treatment and care, say around $240 million.
It’s tremendous that a lot of money is being spent on treating and caring for people who have been infected with HIV. Not all HIV positive people are currently eligible for treatment. Perhaps UNAIDS’ claim that 60% of those who are eligible were on treatment at some time, although the figure, however many hundreds of thousands it may be, does not discount those who have died or who have been otherwise lost to follow up.
Around 95% of Tanzanian people are HIV negative. Out of the 1,470,000 people who are living with HIV, between one and two thirds may be on treatment. That’s 1-2% of Tanzanian people, at the most. So how do those who control the money decide how to spend the approximately $80 million in order to reduce transmission of HIV; what kind of prevention activities should be prioritized among those 46,300,000 Tanzanians who are still uninfected?
UNAIDS has a slogan (aside from their ‘three ones’ slogan alluded to in the title above) that goes ‘know your epidemic – know your response’. This makes it sound like UNAIDS believes that there are different epidemics in each country, and perhaps even different subepidemics within each country. But their response is always to treat HIV epidemics in Africa as if they are all virtually the same, although they may vary in intensity: but they are all assumed to be ‘driven’ by heterosexual behavior.
It’s not very clear how far $1.70 per head can go towards ‘changing people’s sexual behavior’, but that hasn’t stopped UNAIDS and other big players in the HIV industry (and some of them are very big players indeed) from trying. Billions have been spent on wagging fingers at rooms full of adults and children over the almost 20 years of UNAIDS’ existence.
Luckily there are a few things that can be done to help establish that HIV is probably not entirely heterosexually transmitted and that most finger-wagging exercises are a complete waste of money (their inherent paternalism is probably not considered to be a disadvantage; perhaps neither is their clearly demonstrated ineffectiveness).
For example, in Tanzania (and most other countries) there are only a few places where HIV prevalence is really high. Here’s a list of prevalence by region (the five with the lowest prevalence are the Zanzibar archipelago):
Njombe 14.8
Iringa 9.1
Mbeya 9
Shinyanga 7.4
Ruvuma 7
Dar es Salaam 6.9
Rukwa 6.2
Katavi 5.9
Pwani 5.9
Tabora 5.1
Kagera 4.8
Geita 4.7
Mara 4.5
Mwanza 4.2
Mtwara 4.1
Kilimanjaro 3.8
Morogoro 3.8
Simiyu 3.6
Kigoma 3.4
Singida 3.3
Arusha 3.2
Dodoma 2.9
Lindi 2.9
Tanga 2.4
Manyara 1.5
Mjini Magharibi 1.4
Kusini Unguja 0.5
Kusini Pemba 0.4
Kaskazini Pemba 0.3
Kaskazini Unguja 0.1
And there are further generalizations that can be made about HIV in Tanzania. Prevalence tends to be higher among females, urban dwellers, wealthier people, people with higher levels of education and employed people. It tends to be lower among men, rural dwellers, poorer people, people with lower levels of education and unemployed people.
UNAIDS tends to ‘analyze’ these features, which are shared by all high HIV prevalence countries, and conclude that wealthier, urban dwellers with jobs have bigger ‘sexual networks’ (etc) as if every person with HIV must have a ‘sexual network’ (etc). But there are other figures they could avail of when they are in an analytical frame of mind.
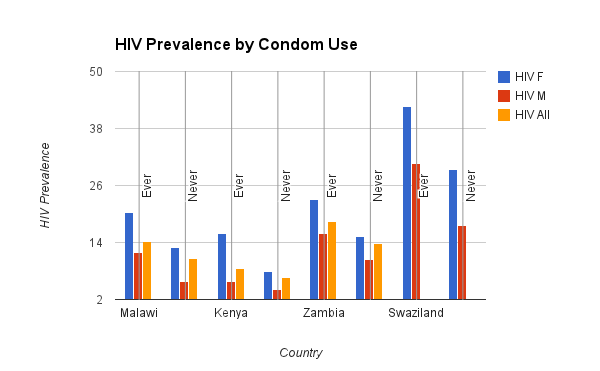
For example, while women are said to be more susceptible to HIV infection for various biological reasons, wealthier, urban dwelling, better edcated women with a job are also much more likely to attend ante natal clinics (ANC) and seek the assistance of some kind of trained health professional when they are giving birth.
Now, you might expect women who attend ANCs and have assisted deliveries to be less likely to be infected with HIV, but you’d be wrong. In many instances they are more likely to be infected, sometimes a lot more likely. Indeed, some countries with the highest HIV prevalence figures also have the highest ANC and attended birth figures, Swaziland, Lesotho, Namibia and Zimbabwe, for example. The contrary tends to be true of low prevalence countries in sub-Saharan Africa.
This is not to say that HIV is never transmitted through heterosexual sex, or that it is always transmitted through unsafe healthcare (even among women). It’s just a clear indication that we need to know exactly what contribution heterosexual behavior makes to epidemics, and what contribution may be made by non-sexual routes, such as unsafe healthcare, cosmetic care and perhaps other practices.
The whole concept of a UN agency set up to ‘fight’ one disease is bad enough. But it’s a whole lot worse if they and the rest of the industry continue to squander precious resources on poorly targeted and ineffective interventions. Resources need to be spent on health, defined as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” (there’s no irony intended in citing WHO here).
Apparently one third of all aid in Tanzania is being spent on HIV, which leaves the other two thirds to be spent on other development areas. So perhaps some of that will eventually be used to address the many poorer, less well educated, jobless people living in rural areas with virtually no infrastructure or social services, but who are HIV negative. They will likely remain negative if even a fraction of available donor funding is spent on working out the relative contribution of unsafe healthcare to the worst HIV epidemics in the world and addressing this issue, however belatedly.