At the beginning of this month, David Gisselquist took a careful look at UNAIDS’ ‘Modes of Transmission’ model and found it seriously lacking, grossly overestimating HIV transmission among couples in long term relationships in Malawi. As a result of this flaw, the model gives results which appear to support the extremely racist view that most Africans in high HIV prevalence countries, male and female, engage in a lot of unsafe sex, and mainly sex with people other than their partners.
David shows how the Modes of Transmission model currently estimates that 81% of Malawi’s 95,000 new HIV infections were accounted for by spousal transmission. If you remove the flaw, the percentage goes down to 20%, leaving 60% of all infections unaccounted for by the model (non-sexual transmissions from mother to child make up much of the remainder). How were all those other people infected, including the women who are said to have infected their babies?
It is very likely that a substantial number of HIV infections in Malawi and other high prevalence countries are a result of non-sexual transmission, such as through unsafe healthcare, cosmetic procedures and traditional practices. The much lauded ‘ABC’ (Abstain, Be faithful, use Condoms) approach to HIV prevention does not work, not because many Africans actually live up to the stereotypical ‘all men are bastards, all women are hapless victims’, but because HIV is not always transmitted through heterosexual sex.
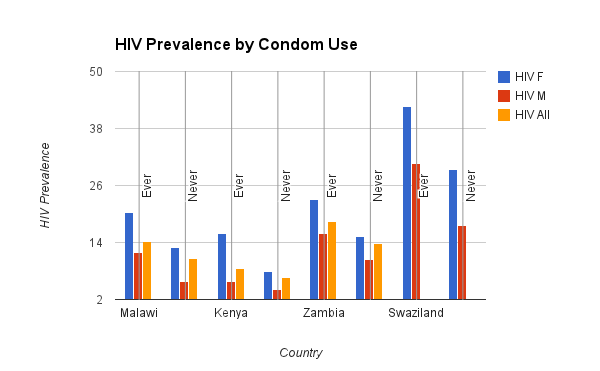
Consider condoms, which are a great technology for reducing unplanned pregnancies, many sexually transmitted infections and sexually transmitted HIV, through anal and vaginal intercourse. But a number of surveys have found that HIV prevalence is very high among those who use condoms. Indeed, prevalence is often higher among those who at least sometimes use condoms than among those who never use them. The following chart is from the relevant Demographic and Health Survey for four countries.

In some cases, HIV prevalence is 50% higher among those who sometimes use condoms than among those who never use them, sometimes 100%. Shocking? Only if you think HIV transmission in high prevalence African countries is all about sex. Consider another set of figures, this time for condom use at last sexual intercourse in past 12 months. The figures for those who have not had sex in the past 12 months also raise questions (data from DHS surveys). You could suggest that people are not honest, or that people who are infected are ‘abstaining’, but it is far more vital to figure out exactly how people are being infected in order to prevent further infections.

Why are HIV prevalence figures so much higher among people who say they sometimes use condoms? I can only tell you what I think; condom use is completely irrelevant to non-sexually transmitted HIV. That sounds obvious, but UNAIDS insist that almost all transmission is through heterosexual sex, yet they stand by figures like these. It is not possible for HIV prevalence to be so much lower among those who never use condoms if almost all HIV transmission is sexual. But there may be an explanation for why those who sometimes use condoms seem so much more likely to be infected.
HIV prevalence is often highest among wealthier, urban dwelling, employed, female, better educated people who live in wealthier countries that have reasonable access to reproductive healthcare services, a relatively low population density and sometimes a higher urban population (but not always). People who answer that description, people who can tick at least some of those boxes (some of the factors are interdependent), it seems, are also more likely to use condoms.
So it is not a case of people with the above characteristics using condoms, yet still being more likely to be infected with HIV, but rather a case of those same people being more likely to be infected with HIV through unsafe healthcare or some other non-sexual route. Once you challenge the sexual behavior paradigm the rest is clear: condoms are irrelevant to non-sexual HIV transmission. It only sounds unintuitive if you keep clinging to the sexist, racist and extremely dangerous reflex about sexual behavior, so beloved by UNAIDS, WHO, CDC, PEPFAR, the Gates Foundation and various universities that have been prominent in the HIV industry.
Given what we so often hear about HIV being inextricably linked with poverty, unemployment, lack of education, isolation, poor access to health services, etc, it is worth emphasizing that the virus may often be more closely linked to the opposite of these factors. Of course, all of these factors are abhorrent and it should be the aim of every wealthy country to ensure that such conditions are alleviated. But if HIV is being transmitted through unsafe healthcare and other routes, all healthcare development must be SAFE healthcare, all HIV education must include information about non-sexual transmission, all employment and environments must exclude risks of bloodborne transmission of HIV, as much as possible.
So first we need to recognize that HIV is not solely transmitted through ‘unsafe’ sex and that it can be transmitted, perhaps far more easily, through unsafe healthcare, cosmetic procedures and traditional practices. ABC ‘strategies’ do not work because HIV transmission is not all about sex, not because Africans are too careless, promiscuous or ignorant (or even ‘disempowered’) to follow its patronizing advice. Safe sex has its place, but safe healthcare is a far more urgent issue in high HIV prevalence African countries right now. It’s not condoms that are failing to protect people against HIV, but the intransigence of UNAIDS and the rest of the HIV industry.