Wajir is a city and county in Kenya’s former North Eastern Province. From a HIV perspective, the county stands out for having the lowest prevalence of all Kenya’s 47 counties, currently estimated at 0.4%. The next highest counties are Mandera (0.8%) and Garissa (0.9%). Wajir, Mandera and Garissa make up what was the province, formerly a part of Jubaland, in Southern Somalia.
Homa Bay is a town and county in the south west, formerly part of Nyanza Province, and the number one county for HIV prevalence, 26%. Indeed, the only counties with prevalence above 10% are Siaya (24.8%), Kisumu (19.9%), Migori (14.3%) and Homa Bay, which (along with Kisii and Nyamira) made up Nyanza. That accounts for one third of all HIV positive people in Kenya.
The question of why HIV prevalence is so high in certain parts of Kenya is usually answered, implicitly or explicitly, with half baked notions about ‘African’ sexual behavior, ‘African’ mores, ‘traditions’, sexual practices, ‘unsafe’ sex, promiscuity. In a word: sex. It’s all about sex, and in the worst hit counties experts have persuaded the US to part with hundreds of millions of dollars for mass male circumcision programs.
A lot less seems to be written about the extremely low HIV prevalence found in the north east. Look up Mandera, Garissa or Wajir on PubMed and you will only come across just over 300 papers altogether, compared to thousands for other locations (and almost 50,000 for Kenya as a whole). But it would be interesting to know how HIV prevalence has remained as low as in many western countries in the north west of Kenya, yet it has risen as high as the worst hit countries in southern Africa in the south west of Kenya.
Sex happens in north eastern counties too. In fact, condom use is generally lower in these counties. Polygamy is more common, as are intergenerational sex and marriage, phenomena the HIV industry sometimes insists are risks for HIV transmission. Knowledge about HIV transmission and how to avoid it tends to be lower in these counties, too. Birth rates are higher than in other parts of the country.
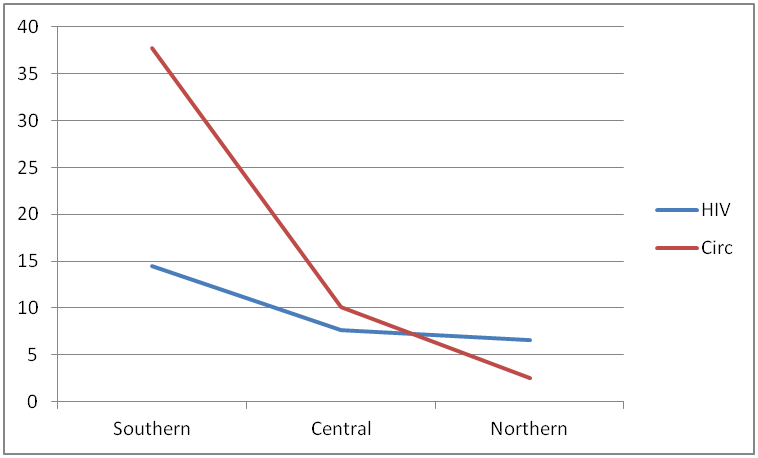
Circumcision is said to be widespread in a number of counties, not just in Wajir (and Mandera and Garissa) but also, for example, in Kilifi. But HIV prevalence in Kilifi is a lot higher, at 4.5%. The populations are predominantly Muslim in both counties, so circumcision is not likely to be the full explanation, nor is religion. There are commercial sex workers and men who have sex with men in every county, with no evidence that these practices are less common in low prevalence counties.
The north eastern counties are, in fact, very different from the rest of Kenya. Kenya was divided up on ethnic lines by the British, which is why the territory once called the ‘Northern Frontier District’ became one province: it was, and still is, populated by ethnic Somalis. They are geographically isolated, in the sense that there are few major roads. Much of the north of Kenya is arid and sparsely populated. Even the Somalis who live elsewhere in Kenya, such as in Nairobi, tend to live in predominantly Somali suburbs.
A similar kind of isolation, albeit on a much larger scale, can be found in northern Africa. The Sahara is sparsely populated and there are few major roads traversing it. HIV prevalence is low in all North African countries. In fact, HIV arrived relatively late in North Africa, and analysis of the common subtypes there suggest that the epidemic spread to a large extent from southern Europe, and to a lesser extent from West and central Africa.
The most common HIV subtype in Kenya is type A, followed by D, with a small proportion of type C. But the most common subtype in the north east of Kenya is type C, this being the most common subtype in southern Africa, Ethiopia and a number of other countries. So the former province really does seem to have a different epidemic or ‘subepidemic’. Type C is known to have evolved later than A and D, so the former North Eastern Province’s subepidemic is newer, like those in North African countries.
But it is still unclear how the above features of certain epidemics and subepidemics are associated with very low prevalence. Instead of looking for phenomena behind very high prevalence in some south western counties, are there certain phenomena that are absent in the north west (and in North Africa)? Isolation doesn’t mean less sex, nor even less ‘unsafe’ sex, and sexual behavior is very poorly correlated with HIV transmission.
We don’t know much about Wajir, Mandera and Garissa because not much research has been carried out there, and it’s not surprising that little HIV research has been carried out where there’s little HIV transmission. But what about other healthcare research? I notice almost all the articles on PubMed are about HIV, and were published in the last 20-30 years. So the area has been isolated from research for a long time.
Now, if there are few roads and limited infrastructures, is healthcare infrastructure similarly limited? It could be expected that access to healthcare facilities is poor and that many people rarely or never go to a hospital, or see any kind of health professional. The majority of women probably give birth at home, coverage of mass drug administration programs, including routine immunizations, is probably lower for these and other more isolated counties.
Borrowing Nicholas Nassim Taleb’s ‘via negativa’ in his book ‘Antifragile’, perhaps HIV prevalence in the north east of Kenya (and in North Africa) has remained low because of infrequent contact with healthcare facilities. This is not to say that healthcare facilities are unsafe in the north east, although it does suggest that they are unsafe in high prevalence counties. Also, it is suggested that HIV is circulating in health facilities, more in some than in others.
Many (including Taleb) like to repeat that ‘absence of evidence is not evidence of absence’. There is a possibility that HIV has been, and is still circulating in health facilities in Kenya, and may account for a significant proportion of infections, perhaps the majority of infections. Little research has been carried out to estimate the relative contribution of healthcare associated HIV transmission. We will never know until the evidence is sought: does limited contact with healthcare keep HIV prevalence low in the north east of Kenya?