The International (formerly African) Network of Religious Leaders living with or Affected by HIV/AIDS (INERELA+) promotes SAVE as a response to Africa’s HIV/AIDS epidemic. SAVE stands for: Safe sexual and skin-piercing behavior; Access to treatment; Voluntary counseling and testing; and Empowerment. This note considers some of the ways that SAVE could strengthen HIV prevention in Africa.
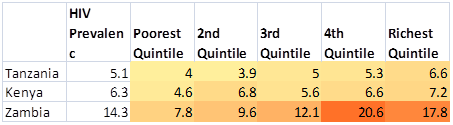
AIDS was first recognized in Africa in 1982. In 2010, 28 years later, the World Health Organization (WHO) estimated that 22.9 million Africans were living with HIV, including 1.9 million with new infections in that year. These infections are not distributed evenly. The people most at risk live in cities in 15 countries, primarily in Southern and Eastern Africa. In these cities, from 20% to more than 50% of men and women aged 15 years today can expect to get HIV at some time during their lives.
Help husbands and wives stop intra-familial HIV transmission
Unlike Western countries, where almost all HIV transmission occurs outside families, a lot of HIV transmission in Africa happens within families – mother-to-child and spouse-to-spouse transmission together account for an estimated 45% of new infections.
(a) Mother-to-child transmission: According to WHO estimates, 390,000 babies in Africa got HIV from HIV-positive mothers in 2010, accounting for an estimated 20% of 1.9 million new HIV infections in Africa in that year (390,000/1,900,000 = 20.5%, rounded to 20%).
(b) Spouse-to-spouse transmission: An estimated 30% of all HIV-positive adults in Africa are married to HIV-negative partners, and the resultant spouse-to-spouse transmission accounts for approximately 470,000 HIV infections per year, equivalent to 25% of all new infections each year (470,000/1,900,000 = 25%). (A note at the end of this blog shows the source of these data and explains this estimate.)
Most Western experts continue to identify high risk groups in Africa, as in the US and Europe, according to extramarital sex – prostitutes, clients, truck drivers, and youth are considered to be at high risk because they have more than average levels of extramarital sex. But in Africa, none of these groups defined by extramarital sex has risks as high as babies born to HIV-positive mothers (without treatment, 35% are infected in 2 years) or spouses not aware their partners are HIV-positive partners (8% per year). In other words, the term “high risk groups” in Africa applies first and foremost to persons with intra-familial risks.
With good information and with some medical assistance husbands and wives can work together to stop 700,000 infections per year – reducing mother-to-child transmission by 320,000 (from 390,000 to 70,000) and spouse-to-spouse transmission by 380,000 (from 470,000 to 90,000; see the note at the end of this blog). This would reduce total HIV transmission from all causes by 37% – from 1.9 million to 1.2 million infections per year. There are two major challenges to achieve this outcome.
The first challenge is to reform and extend couple counseling. A lot of men and women don’t think they could have HIV because they and their partner have had very conservative sex lives. Many women who test HIV-positive are afraid to tell their husbands and/or assume they got it from their husbands, so there is no reason to tell them. The best way to overcome these testing problems is to make it clear – both in public messages as well as in counseling – that a lot of HIV in Africa comes from blood exposures. This is important for couples to know – it means an HIV infection is not a reliable sign of sexual behavior. It also means that conservative sexual behavior provides no assurance that anyone is HIV-negative.
It will take some work to get people to realize that their own or their spouse’s HIV infection might well have come from a skin-piercing event, because this realization has to overcome several decades of stigmatizing and misleading half-truths – blaming victims for their infections rather than acknowledging that unsafe health care has been an important part of the problem.
Once husbands and wives can go get tested and talk with each other about their HIV test results without distrust and blame generating family crises, then couples will be better able to plan for what to do to protect babies and uninfected spouses, and to care for those who are infected. Aside from changing messages to de-link HIV from sex, testing should be readily available, with or without counseling. People should be able to buy kits to test themselves (as in South Africa). Opt-out testing is a good way to go. However, compulsory testing is almost always a bad idea.
The second challenge is for governments and donors to prioritize prevention of mother-to-child transmission in allocating scarce resources for HIV prevention. Protecting babies will take a lot of money and medical personnel. This requires: testing pregnant women; testing husbands to get them involved; giving anti-viral drugs to HIV-positive women and their new babies; and helping HIV-positive mothers wean early (after 6 months is a common recommendation, but some may want to do so earlier or later). With these interventions, infected mothers will infect less than 5% of their babies, which would cut the annual number of infections from mother-to-child by an estimated 320,000 (from 26% to 4.5% of babies born to 1,490,000 HIV-positive mothers). Even lower rates of mother-to-child transmission can be achieved with anticipated new drugs or other options.
Whereas preventing mother-to-child transmission requires substantial assistance from outside the family, once husbands and wives know one of them is HIV-positive, they can protect the HIV-negative partner with little or no outside assistance. Condoms are almost 100% effective against sexual transmission (some studies reporting lower efficacy did not consider that condom-users might have gotten HIV from bloodborne risks). If the HIV-positive partner is eligible for antiretroviral treatment and achieves a low viral load, unprotected sex may be safe. If the wife is HIV-positive, circumcising the husband might reduce his risk, but he would not be safe without other protection (eg, condoms). Couples must also take care to avoid blood-to-blood contact through shared razors, toothbrushes, syringes and needles, etc.
Stopping HIV from getting into families
Extra-familial HIV transmission threatens families as well. Some men but many more women get HIV before they are married and bring it into the marriage. But that’s not all – even among old married couples, most couples with HIV are discordant. Husbands and wives continue to import HIV into marriages. According to Western ideas about HIV epidemics that have been imposed on Africa, all these infections come from sex. But those ideas don’t fit facts. Surveys find a lot of HIV in babies with HIV-negative mothers, in young and old virgins, and in men and women married for years with no outside partners and an HIV-positive spouse.
The best way to protect families from outside risks is to warn them about all risks, from blood contacts as well as from sex. African governments could improve these warnings by belatedly asking researchers and investigators to trace a lot of HIV infections to their source to see what risks are infecting babies, young women, etc — including especially people with limited and no sexual risks.
Conclusion: focus on the family
Whereas HIV in the US and Europe has been a tragedy for men who have sex with men and has largely avoided families, in Africa it hits families hard – weakening and killing husbands and wives, interfering with child-bearing, killing babies, taking huge expenses for treatment, and threatening family trust.
African families are strong and can carry much more of the burden to fight the epidemic. To do so, they need honest information – that an unknown but important proportion of infections comes from unsterilized instruments in health care and cosmetic services. Such messages not only allow people to see and avoid risks, but also make is easier for husbands and wives to test and to share HIV test results – the foundation for intra-familial HIV prevention.
Enlisting families to cut intra-familial transmission and supporting them with programs to prevent mother-to-child transmission could cut HIV transmission in Africa by an estimated 700,000 infections per year (37% of total transmission). This can be achieved with available budgets and personnel; but because these resources are limited, governments and donors would have to prioritize. One program that competes for money and personnel asks for $1.5 billion–$2.7 billion and several thousand surgical teams to circumcise 20 million men by 2015. Critics argue, inter alia, that condoms are more reliable. But even if one ignores the critics, circumcision looks like an expensive distraction: even advocates estimate the 20 million circumcisions would reduce annual HIV transmission by less than 200,000 (10% of total transmissions) in 2015 – far less than can be achieved with the intra-familial focus proposed in this note.
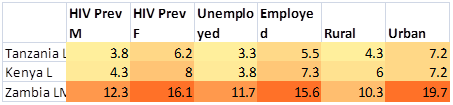
Statistical note: According to WHO, 19.8 of the total 22.9 million Africans living with HIV in 2010 were adults (page 210 of this link). From national surveys in several dozen African countries over the last decade, the percentage of adults with HIV who are married ranges from roughly 53%-77% for men and 49%-69% for women (see Table below). From the same source, the percentage of adults with HIV who are married to HIV-negative partners ranges from roughly 10%-25% in the worst epidemics in Southern Africa to 25%-35% in mid-range epidemics in East Africa, to 50% in countries with low level epidemics (see Table below).
From these data, an estimated 5.9 million HIV-positive adults (30% of 19.8 million adults) are married to HIV-negative spouses. In studies that followed discordant couples who were not aware of their infections, approximately 8% of HIV-positive partners infected their spouses each year. Thus, 5.9 million HIV-positive adults in discordant couples infect an estimated 470,000 spouses each year (0.08 x 590,000 = 470,000). Assuming that expanded testing and couple counseling reaches all discordant couples, and that they use condoms and take other precautions to cut spouse-to-spouse transmission from 8% to 1.5% per year, this would reduce annual spouse-to-spouse HIV transmission in Africa by 380,000 per year, from 470,000 to 90,000.
Table: HIV in adults, married adults, and married adults with HIV-negative partners (selected countries in Africa)
| Country year |
Sex |
% adults who are HIV+ |
% HIV+ who are married |
Among married HIV+ people, % with a spouse who is HIV- |
% of HIV+ people with a spouse who is HIV- |
| A |
B |
C = AxB |
| DR Congo 2007 |
Men |
0.9 |
53 |
75 |
40 |
|
Women |
1.6
|
66
|
85
|
56
|
| Burkina Faso 2003 |
Men |
1.9 |
75 |
70 |
53 |
|
Women |
1.8
|
68
|
70
|
48
|
| Ethiopia 2005 |
Men |
0.9 |
77 |
73 |
56 |
|
Women |
1.9
|
54
|
77
|
42
|
| Ghana 2003 |
Men |
1.5 |
75 |
62 |
47 |
|
Women |
2.7
|
67
|
60
|
40
|
| Tanzania 2007-08 |
Men |
4.6 |
70 |
58 |
41 |
|
Women |
6.6
|
59
|
53
|
31
|
| Uganda 2004-05 |
Men |
5.0 |
72 |
45 |
32 |
|
Women |
7.5
|
50
|
35
|
18
|
| Kenya 2008-09 |
Men |
4.3 |
67 |
47 |
31 |
|
Women |
8.0
|
49
|
53
|
26
|
| Mozambique 2009 |
Men |
9.2 |
74 |
52 |
39 |
|
Women |
13.1
|
60
|
51
|
31
|
| Zambia 2007 |
Men |
12.3 |
56 |
45 |
25 |
|
Women |
16.1
|
69
|
37
|
26
|
| Lesotho 2009 |
Men |
18.0 |
65 |
33 |
21 |
|
Women |
26.7
|
53
|
28
|
15
|
| Swaziland 2006-07 |
Men |
19.7 |
54 |
21 |
11 |
|
Women |
31.1
|
43
|
23
|
10
|
Source: data are from country surveys available at this link; click on the country, and then on DHS (Demographic and Health Survey) or AIS (AIDS information surveys.