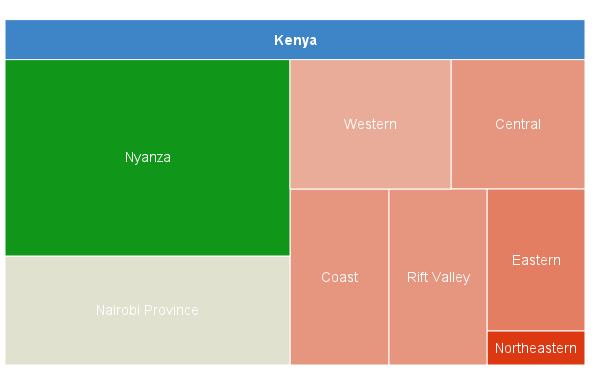
Why is HIV spread so unevenly? In some parts of Kenya prevalence is at ‘hyperendemic’ levels, over 20%, almost 30% in one county. Yet in other counties it is low, 1% or lower. If, as we are constantly told, 80%, even 90% of HIV transmission is a result of unsafe sex (most of the remaining 10-20% being a result of mother to child transmission), what amazing sex lives people in some counties must have (or disgraceful, if you prefer). And what dull (or worthy) lives those in other counties must have, apparently only having sex for the purpose of procreation.
If, on the other hand, HIV is not always a result of sexual behavior, if many people may be infected through unsafe healthcare, even unsafe cosmetic and certain traditional practices, some of the factors involved in HIV transmission rates, low or high, start to make a lot more sense. The list of factors is long (over 40), but the italicized paragraphs are the kind of explanations given by the ‘it’s all about sex’ camp, so they are mostly the same. Yes, some HIV transmission is a result of sexual behavior, nobody is denying that, but some is not. Also, some areas where HIV transmission is high are in need of further study; a priori explanations for high and low prevalence have no place in science (though they seem to receive a warm welcome in a lot of papers on HIV epidemiology).
Christian
Prevalence is often higher among Christians than Muslims, and generally among males than females; not sure why this is so; the majority of HIV positive people in the world live in predominantly Christian countries, meaning that a lot more Christians than non-Christians are infected; why this is so is not clear, although both healthcare access and HIV prevalence are noticeably low in some Muslim dominated countries
Men less likely to be circumcised; also Christians are ‘less restrained’ in their sexual behavior than Muslims
Circumcision
There is no clear evidence that circumcision reduces HIV transmission and it could only influence sexual transmission, at best; however circumcision is risky if carried out in unsafe healthcare facilities or in traditional settings
Circumcision ‘cleaner’ or ‘more hygienic’, although this is a hypothesis, there is no unambiguous evidence
Colonization
The vast majority of HIV positive people live in countries that were colonized by the British. This may relate to healthcare facilities, access to healthcare, health seeking behavior, infrastructure, stability, etc
It’s somehow related to sex
Condom use
HIV prevalence is higher, often far higher, among people who sometimes use condoms than among those who never do, suggesting that HIV risk is not always sexual
Those who are already infected are more likely to use condoms
Culture
Cultural practices such as female genital mutilation (FGM) may increase the risk of being infected, although it increases both sexual and non-sexual risks; yet prevalence among people who practice FGM is generally low, which suggests that there are other factors involved
Increases HIV transmission; if prevalence is low this can be explained away by reference to attitudes towards extra-marital sex, etc
Depo Provera
Increased risk for women taking it and for their partners
Denies that this is a risk and claims that the benefits (prevent conception) outweigh any disbenefits, which don’t exist anyway
Education
Educated people may have better access to healthcare and be more likely to use healthcare
Educated people have access to bigger sexual networks
Employment status
People with a job can afford healthcare, although this may not be safe healthcare; jobs may include healthcare or health insurance; some occupations provide healthcare services;
People with a job have more money and therefore access to bigger sexual networks; despite prevalence generally being higher among employed people, some suggest that unemployed people have little else to do but have sex
Female
Prevalence is usually higher among women, possibly because they have more need to use healthcare services, especially when pregnant and giving birth; they are also more susceptible to sexual transmission
Women are more vulnerable and have less power to make choices; they are usually victims, otherwise they fall under one of the many categories of sex worker
Fertility
Higher fertility may increase healthcare exposure, although it is often associated with low prevalence areas, rural areas, etc
Higher fertility means more unprotected sex
Healthcare
Healthcare may not always be safe, which may explain why countries with good access to healthcare for everyone, such as Botswana, may result in higher HIV prevalence
Sick people, including people with HIV, seek healthcare, which is why healthcare may seem to be associated with higher HIV prevalence; this is especially true of STIs
Hepatitis
HBV and HCV are much more likely to be transmitted through non-sexual routes, such as unsafe healthcare, cosmetic and traditional practices, also injection drug use
Presence of HBV and/or HCV are signs that the person is either promiscuous or an intravenous drug user (or both)
Herpes
Rates can be extremely high in some populations because it is very easy to transmit, sexually and through other routes; it plays a role in being infected with and transmitting HIV but the role is complex
It is a sign that people infected engage in unsafe sex and increases risk of transmitting and being infected with HIV
Inequality
It is neither clear that inequality is associated with higher risk, nor why this may be so
People are more vulnerable to sexual risk, especially women
Infrastructure
Good infrastructure is often associated with high HIV prevalence, which may suggest better access to unsafe healthcare
Good infrastructure gives access to bigger sexual networks
Male
Prevalence is usually lower among men than women, which leaves a question mark over instances of higher prevalence among men when they are found, for example, Muslim men in Kenya; prevalence may be lower because of lower use of health facilities
Men are considered to be mere spreaders of sexually transmitted disease, whether they are rich or poor, urban or rural dwelling, etc
Marriage
Sometimes HIV prevalence is far higher among married than unmarried people and it is not clear why
Married people are less likely to use condoms; they also have extra marital sex, usually the men, then they go home and infect their spouse
Migration
Migration can be for work, which may involve work-related healthcare, which may be unsafe and may not be subject to levels of scrutiny faced by public facilities, however scrutinized they may be
Migrants, being away from home, either have other sexual partners or visit sex workers; they then return home to infect their spouse
Mobility
Possibly increases access to health facilities, but mobility on it’s own doesn’t seem to explain high prevalence
Mobile people have access to bigger sexual networks
Muslim
Figures vary, with prevalence higher among Muslims than Christians in some countries (eg, Burundi, Rwanda, Mozambique, but not Kenya or Tanzania), also higher among Muslim men than women in others, eg Kenya; not sure why this is so
Men more likely to be circumcised; also Muslims are ‘more restrained’ in their sexual behavior than Christians
National borders
High HIV prevalence has been reported at border areas in the past and rates of unsafe sexual behavior may be higher; but the sex workers and long distance drivers who are said to be responsible for high rates have often taken part in STI eradication programs and may frequently use STI clinics
Long distance drivers have sex with sex workers, then they go home and have sex with their spouses
Occupation – armed forces
Members are unlikely to have any option as to whether they take part in various health programs, tests, etc; healthcare is likely to be free, which means usage is also probably higher
They have access to bigger sexual networks and frequently visit sex workers
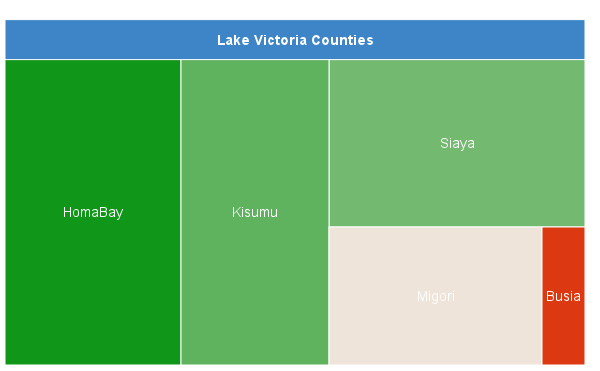
Occupation – fishing
Prevalence is high in fishing communities, not necessarily highest among the fishermen; also, very high prevalence seems to be a feature of only some fishing communities, especially lakes; not sure why HIV prevalence is so high
Fishermen do risky work, therefore they are not bothered by sexual risk; also, they spend a lot of time away from home; also, they use sex as a bargaining tool
Occupation – mining
Artisanal mining is not so much associated with HIV so this probably applies to industrial scale mining; the work-related healthcare to which miners have access (they may even be compelled to receive certain health services and tests) may not be safe
Miners work a long way from home and don’t see their family much so they have extra-marital relationships and/or visit sex workers, then go home and infect their spouses
Occupation – teaching
Prevalence has been claimed to be higher and lower among teachers, at different times and places; they probably face similar risks to other public sector employees, whatever those may be
Teachers frequently have sex with their pupils (which may be true, and should be addressed, but it may turn out to have little to do with HIV transmission)
Occupation – transport
Transport workers may use health facilities more; also, they may have been persuaded to take part in STI eradication programs as they have been blamed for all sorts of things; these STI programs may not always have been safe
Transport workers are mobile, which means they have access to bigger sexual networks; then they go home and infect their spouses
Polygamy
Sometimes associated with higher transmission, sometimes with lower transmission, therefore not clear. It is not only practiced by Muslims but also by some tribes and even at least one Christian sect in Kenya
When prevalence is higher, this is because polygamy involves ‘concurrency’; when lower, it’s because men with more than one wife don’t need to have extra-marital sex, or not as much
Population density
Increases pressure on health facilities
Said to increase the size of sexual networks
Population growth
Increases pressure on health facilities
Said to increase the size of sexual networks
Poverty
HIV prevalence is often lower among poorer people, suggesting that they may face lower risk from, for example, unsafe healthcare because of reduced access; however, being poorer means that the only healthcare available may be unsafe
If prevalence is high, poorer women are more vulnerable (to sexual transmission) for various reasons; if it’s lower, poorer people are less likely to be part of a ‘sexual network’ or their networks are likely to be smaller
Prisoners
There may be some kind of drug use that involves cutting or skin piercing (seems unlikely injection drug use would be common); healthcare is unlikely to be very comprehensive or safe; tattooing and traditional medicine may be additional risks, perhaps also scarification, blood oaths, etc
They have sex with other prisoners, the implication being that the sex includes anal sex; and/or injected drugs or drugs that involve skin piercing; condoms are usually not permitted
Rural
Rural dwelling people have less access to health facilities and infrastructure, which may go some way to explaining why prevalence is usually lower in rural areas
Rural dwelling people have access to smaller sexual networks
Schistosomiasis
This has been shown to increase susceptibility to infection and onward infection, which suggests that some people have sex, not very surprising; but endemic schistosomiasis, which is very cheap to treat, suggests weak healthcare systems
Lots of people having lots of sex with lots of other people all the time: schistosomiasis only adds to what is a ‘known issue’
Sex work
Prevalence among sex workers is low among some sex workers in Western countries unless they also engage in injection drug use but their biggest risk in countries with unsafe healthcare could be their frequent exposure to STI clinics and STI eradication programs; also, a lot of what is referred to as ‘sex work’ is in fact sex between people who are in a relationship or married; many people who are related, in a relationship or married also do business with their partner or relative; ‘gift giving’ is sometimes said to be a form of ‘transaction’ between two people who have sex; this is a very stigmatizing use of the term ‘sex work’ (a bit like the term ‘orphan’, which refers to children in developed countries who have lost both parents, but children who have lost one parent in developing countries; or the word ‘trafficking’ which seems to refer to just about anything that involves sex and that can attract funding to ‘rescue victims’ from)
Sex workers are forced into sex work by poverty, powerlessness, vulnerability, etc, but their consequent risks are high and entirely sexual, unless they are also injection drug users
STIs
STIs do not only suggest unsafe sexual behavior, they also suggest a health system that is failing; some are also transmitted through non-sexual routes, such as herpes and HIV
STIs are a sign that a person engages in unsafe sex
TB
TB is likely to be an occupational disease in deep mines, though mining operations deny this, as they don’t want to compensate those who contract it, pay for their treatment or improve conditions in mines; it increases HIV transmission in both directions
HIV positive people are more susceptible to TB
Tribe
Prevalence is high in some tribes and low in others (high among Luos, low among Somalis in Kenya, for example), which suggests that there may be several factors involved; there are ‘risky’ practices in tribal groups among whom HIV prevalence is low, as well as high (for example, female genital mutilation, which is widespread among Somalis)
‘Tribal’ practices and/or ‘traditional’ practices can be wheeled out on any occasion, either to explain high prevalence or low prevalence; they often involve sex or some form of brutality an are generally inflicted by men on women
Urban
Urban dwelling people have easier access to health facilities and other infrastructure
Urban dwelling people have access to bigger sexual networks
War/civil conflict/refugee camps
Prevalence is generally low during wars and only increases after the war has finished, perhaps because health seeking behavior changes during wars, health facilities become less accessible, money is short, infrastructure is destroyed, etc
If HIV is transmitted it is because people take advantage of the situation, rape and other forms of sexual violence being common; but as prevalence is usually lower it is claimed that sexual networks become smaller, people return to rural areas, etc
Wealth
Prevalence is often higher among wealthier people, suggesting that they may use healthcare more frequently; they may also face occupation related risks that are also non-sexual
Wealthy people can become part of larger sexual networks; they have more opportunities for sex and are more likely to avail of these opportunities
Widowhood
Prevalence among widows and widowers can be very high but it is not clear why
Widows are, in some cultures, inherited, having been widowed because their husband (obviously) died of AIDS; they are ‘cleansed’ (have sex with their inheritor) who may be the brother of the deceased, and infect him; he goes on to infect his other partners, including his spouse
The list above makes no claim to be exhaustive. When there is so much diversity in HIV epidemics within and between countries, why would anyone conclude that almost every factor is, ultimately, a matter of sexual behavior, or somehow relates to sexual transmission? It’s no wonder, given the above list, that HIV positive people are feared, even despised. It is the view that transmission is almost always sexual that results in the stigma UNAIDS and other institutions claim to abhor and pretend to be fighting; they are the source of the stigma. HIV ‘prevention’ programs that include some or all of the italicized arguments above merely spread the stigma.